[I am quite sure that this post will attract some response from the DRE community. If you comment, I will print it provided it does not have curse words or is an ad hominem attack with no substantive merit]
When those who defend the motorist accused are confronted with a DUID case and where there is a Drug Recognition Expert (DRE) who renders an opinion, frequently the thought may naturally be for them to cross-examine from a point of view of strict compliance to the DRE protocol. There is a basic issue of the validity of this defense strategy. In following this course of action, one is legitimizing the concept of DRE.
In general there are two types of typical scenarios that may employ a DRE officer:
- The motorist is stopped by a non-DRE. The person is reasonably detained at the scene for a DRE who is called to the scene to do an investigation. This one is rare. Doing a DRE examination is impossible to do at the roadside. I don’t mean it is difficult. I mean it is not possible to do at roadside.
- The motorist is stopped by a non-DRE. The motorist is arrested for suspicion of DUID without a DRE at the roadside. Then it becomes the good old fashioned probable cause (PC) determination for the particular arrest decision. This is why, in my opinion, a defense attorney can never legitimately waive a DUI or DUID case into court. It is incumbent on the defense in these cases to get that arresting officer or trooper to commit to the reason for the arrest. Make the undertrained, non-DRE officer get specific. Ask them for the basis of their knowledge as to how the perception/observation they made is traceable to the drug and how it is indicative of impairment. Then, the defense attorney should develop how the arresting officer has no formal educational background in DUID, meaning that he or she is not a pharmacologist, a medical doctor or a clinician. Also expose how the arresting officer likely has no university level scientific education. The defense attorney should establish how that officer has no police training in DUID (such as the battery of NHTSA courses such as ARIDE, Drugs that Impair Driving, DEC or DRE). Then, the defense attorney exposes the arresting officer’s actions for what he or she is really doing which is guessing at the time of the arrest. Guessing is far from PC. Remember a post-arrest DRE process can never justify an arrest. PC has to precede arrest.
Why not use a credentialed pharmacologist instead to examine the validity of the particular opinion of the DRE opinion? Why give legitimacy to the Drug Recognition Expert (DRE) program by looking at strict compliance?
What is a pharmacologist and what is pharmacology?
A pharmacologist comes in two varieties: a PhD (an academic degree) and a PharmD (a professional degree).
There are two major employment sub fields for pharmacologists: (1) theoretical drug development, and (2) clinical pharmacology.
Pharmacology is firmly rooted branch of science. As a formal scientific endeavor, it dates back to the early 19th century. The first formal university chair in pharmacology was established in 1847. Pharmacology is generally referred to as the study of a drug’s interaction with a living organism. For our purposes (i.e., DUID), there are 3 relevant subsets of pharmacology:
- Pharmacodynamics which is study of the drug’s effect on the person (e.g., effective therapeutic dose, impairment, toxicity)
- Pharmacokinetics which is the study of the time course of the drug through the compartments of the human being (i.e., Absorption, Distribution, Metabolizing, and Elimination)
- Pharmacogentics is the study of environmental or genetics on pharmacology
How does this differ from a DRE?
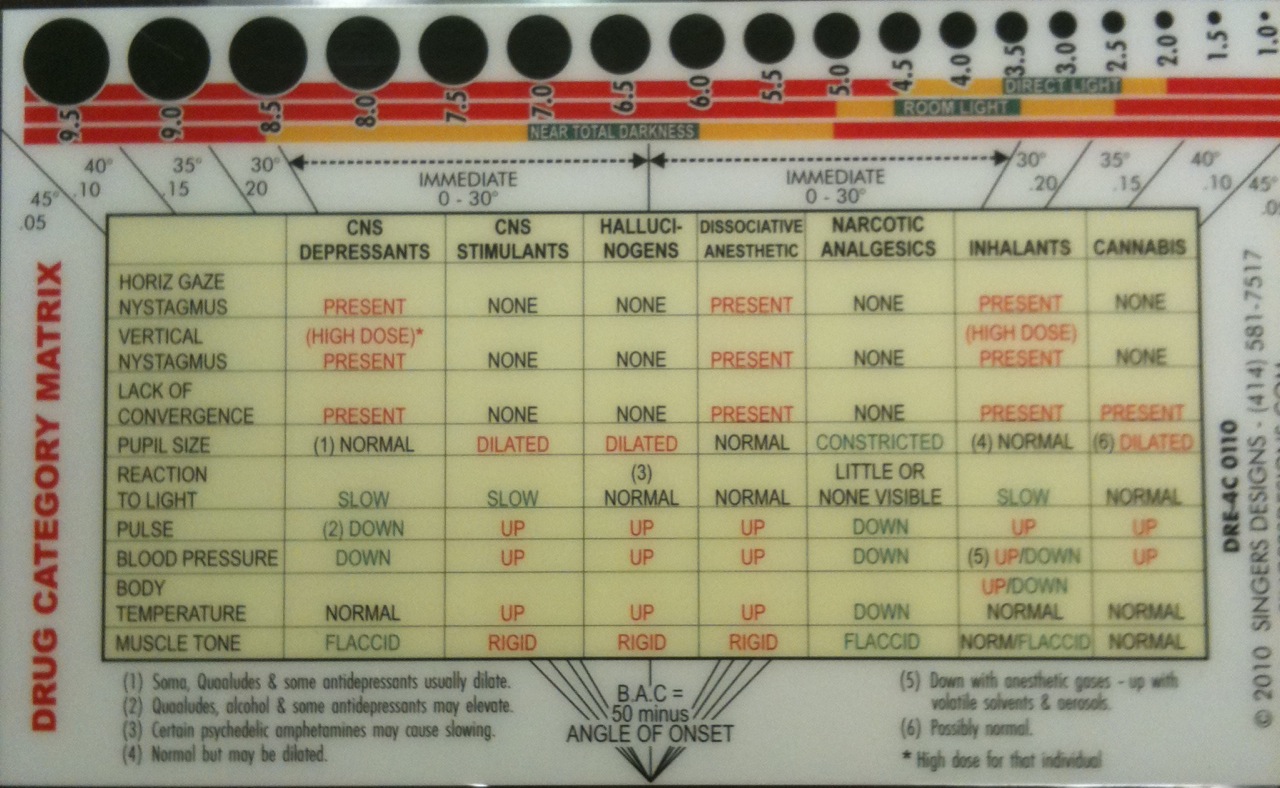
On the other hand there is the DRE officer. According to the DECP website, it originated out of observations from police that lead to consultations by them to those in the scientific field. It was recognized by the LAPD in 1979. The DRE is a non-credentialed, dangerously, and incorrectly trained lay person who is opining what in reality is a very complicated multi-variable pharmacodynamic opinion. Frequently, the DRE presents this opinion in court as a conclusion. All of the complicated data that is captured is reduced to a binary concept and then shoe-horned into a chart. Follow the chart, they hypothesize, and you get a valid answer every time. Hogwash!
To say that the DRE and the pharmacologist do the same thing is not unlike saying that monkey shot into space and an astronaut do the same thing.
How can a pharmacologist be useful to a jury?
First off, a pharmacologist can render an expert opinion. DREs should never be able to opine an expert opinion. At the very least, a credentialed pharmacologist would be able to totally refute the lay opinion of the Dr. Cop in terms of impairment. This is typically done through three main avenues: (1) a total and complete lack of any sort of validity of the DRE program; according to their own studies there is not even facial validity, and according to peer review studies the correct call of presence of a drug can be worse than a random guess, (2) a fundamental lack of information that the DRE has on the dosing of this person, and other important pharmacological variables as applied to this particular human being, and (3) by performing legitimate interpretive pharmacology derived from therapeutic dosing history and records to prove steady state and not impairment.
On the analytical chemistry side, the notion of opining as to pharmacodynamic effect based upon one data point of an analytical chemistry result is not science, it is science fiction. Most people who testify as to the result of the analytical chemistry (which DREs should never do) have no basis to testify as to pharmacology. The one-dimensional reliance on “one size fits all” reference charts, such as Winek’s “Drug and Chemical Blood Level Data”- 2001 [Fisher Scientific] Forensic Sci Int 122,107,2001; Repetto’s “Therapeutic, toxic, and lethal concentrations in human fluids of 90 drugs affecting the cardiovascular and hematopoietic systems” Clin Toxicol 35,345,1997, and even the venerated Baselt’s “Disposition of Toxic Drugs and Chemicals in Man” is dangerous and unscientific.

 The McShane Firm | DUI Lawyers
The McShane Firm | DUI Lawyers Pennsylvania DUI Blog
Pennsylvania DUI Blog
James T. O'Donnell says:
Well put Mr. McShane,
I am consulted frequently by defendents in DUI-Drug cases based on DRE experts.
Frankly, it is very easy to identify that the DRE can not scientifically establish impairment, especially when the driver is taking chronic medications, and had they impaired the driver, they would most likely have reported the impairment to the prescribing physician.
When consulted by prosecutors, I always advise them to check with a pharmacologist BEFORE they indict; when they don’t, they usually end up dropping the charges after my report is submitted.
James T. O’Donnell PharmdD
Associate Professor of Pharmacology
Rush Medical College
117 S. Cook St.
Barrington, IL 60010
847 769 2843
jim@pharmaconsultantinc.com